REDUCING
INFECTIOUS COMPLICATIONS AFTER TRANSRECTAL PROSTATE NEEDLE BIOPSY USING
A DISPOSABLE NEEDLE GUIDE: IS IT POSSIBLE?
(
Download pdf )
Clinical Urology
Vol. 37 (1):
79-86, January - February, 2011
doi: 10.1590/S1677-55382011000100010
CENK GURBUZ, LUTFI CANAT, GOKHAN ATIS, TURHAN CASKURLU
Istanbul Goztepe Training Hospital, Department of 2nd Urology, Istanbul, Turkey
ABSTRACT
Purpose:
To investigate whether the use of a disposable needle guide results in
a decreased incidence of infectious complication after transrectal prostate
needle biopsy (TPNB).
Materials and Methods: Fifty five patients
who underwent 10-core TPNB were randomized into two groups. A pre-biopsy
blood and urine examination was performed in both groups. Group 1 (25
patients) underwent biopsy with disposable biopsy needle guide and Group
2 (30 patients) underwent biopsy with reusable biopsy needle guide. All
patients had a blood and negative urine culture before the procedure.
The patients received ciprofloxacin 500 mg twice a day beginning the day
before the biopsy and continued for 3 days after. Serum C-reactive protein
levels and urine and blood specimens were obtained 48h after the biopsy.
Primary endpoint of the study was to determine the effect of needle guide
on the bacteriologic urinary tract infection (UTI) rate and secondary
end point was to determine symptomatic UTI.
Results: The mean age of the patients was
63.46 (range 55 to 68) years. There were no significant differences regarding
the prostate-specific antigen level, prostate size, existence of comorbidity
in two groups before the procedure. Bacteriologic and symptomatic UTI
was detected in 4% vs. 6.6% and 4% vs. 3.9% in Group 1 and 2 relatively
(P > 0.05).
Conclusion: The use of a disposable needle
guide does not appear to minimize infection risk after TPNB. Large scale
and randomized studies are necessary to determine the effect of disposable
needle guide on infection rate after TPNB.
Key
words: prostate; biopsy; needle; infection
Int Braz J Urol. 2011; 37: 79-86
INTRODUCTION
Transrectal
ultrasound (TRUS) guided needle biopsy of the prostate is the most common
modality used to diagnose prostate cancer. Since male individuals in a
screening population are asymptomatic, biopsy procedure should be safe
and morbidity should be kept to a minimum. Transrectal prostate needle
biopsy (TPNB) is safe for diagnosing prostate cancer with few major, but
frequent minor complications, such as hematuria and hematospermia (1,2).
Infectious complications after TPNB are an important issue of concern.
Currently, many urologists use prophylactic antibiotic therapy and/or
enemas to minimize infection-related complications; however, such therapy
does not completely eliminate the risk of infection (3). The infectious
complications associated with this procedure include: asymptomatic bacteriuria,
fever, symptomatic urinary tract infections (UTIs), and bacteremia (4,5).
Although many biopsy protocols have been
described to reduce infectious complications after a TPNB, such as modified
bowel preparation, different type and duration of antibiotic prophylactic
schemes, and number of biopsy cores (6,7). The role of a disposable needle
guide to reduce the infection rate has not been adequately assessed. The
notion that biopsy equipment, such as reusable guides, may be important
as a contamination site for bacteremia, was first evaluated by Tuncel
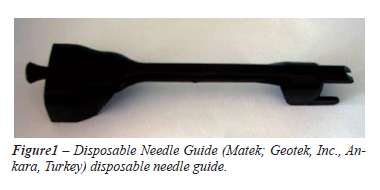
et al. (8). A disposable TRUS-probe needle guide (Matek; Geotek, Inc.,
Ankara, Turkey) has been developed to reduce the possible source of infectious
complications and has been on the market in Turkey for 3 years.
We prospectively investigated whether the
novel disposable TRUS-probe needle guide may decrease infectious complications
after TPNB.
MATERIAL AND METHODS
Between
January and June 2009, 55 patients were included in this study. All participants
gave written informed consent. The local ethics committee approved the
study. The mean age of the patients was 63.46 years (range 58-66 years)
in the present study. The patients in whom TRUS-prostate biopsy was planned
because of elevated prostate-specific antigen (PSA) levels were included
in the study. Exclusion criteria included the following: patients who
had an indwelling Foley catheter, symptomatic or asymptomatic UTIs, bleeding
disorders, acute prostatitis before prostate biopsy, a previous prostatic
biopsy or prostatic surgery, or any antibiotic treatment or anticoagulant
therapy.
A midstream urine culture, serum C-reactive
protein (CRP) level, and WBC count of all patients were obtained two days
before the procedure. The biopsy procedure was performed with the patients
in the left lateral decubitus position using a Toshiba Fabio scanner with
a 7.5 MHz bi-planar probe attached(Toshiba, Tokyo, Japan).
Patients were randomized into 2 groups by
using sealed, opaque envelopes; in Group 1 (25 patients) the biopsy was
performed with disposable TRUS-probe needle guide; and in Group 2 (30
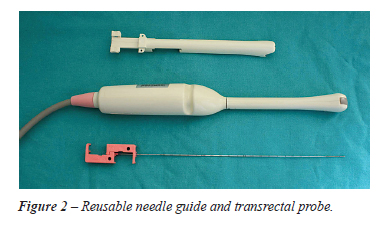
patients) the biopsies were performed with a reusable needle guide. A
completely disposable apparatus of single unit construction designed for
operative use in conjunction with a transrectal ultrasound probe when
performing TPNB are presented in Figure-1. The separable and detachable
features of the reusable needle guide are presented in Figure-2.
Peri-operative prophylaxis included administration of 500 mg of ciprofloxacin
orally the night before the procedure, and an enema per rectum 1 hour
before the procedure. Patients were instructed to continue to take ciprofloxacin
500 mg p.o. bid 3 days after the procedure.
Before the biopsy, a standard condom was
fitted over the distal tip of the TRUS-probe and filled with lubricant
gel. Depending upon randomization, either a reusable or a disposable needle
guide was then fitted over the probe and the first condom. A second condom
was fitted over these items and filled with lubricant gel. All patients
received local anesthesia, consisting of 10 mL 1% lidocaine. Injection
was performed around the neurovascular bundle at the prostatic base and
apical location with an 18 gauge 20 cm needle by inserting the needle
through the needle guide under TRUS guidance and entering Denonvilliers’
fascia. Infiltration was done on each side of the prostate for a total
of 2 punctures. The 10 core prostate biopsies were taken with a spring-loaded
biopsy gun (C.R. Bard, Inc., Covington, GA, USA) and an 18 gauge Tru-cut
biopsy needle. The core sampling notch was approximately 17 mm long by
1.2 mm in diameter. Repeated biopsy specimen collections were performed
using the same needle. The procedure including ultrasound examination
and biopsy required 10 minutes on average.
Upon completion of the procedure, the ultrasound probe was disinfected
by wiping it with a 3.2% glutaraldehyde solution. The reusable needle
guide has two separate pieces which form a lumen after being attached
together. The reusable needle guide was soaked in a glutaraldehyde solution
for at least 30 minutes, then rinsed with sterile saline and wiped off.
UTI was defined as bacteriologic UTI (bUTI):
A patient with a blood or urine culture positive for a known uropathogen
and symptomatic UTI (sUTI): A patient with an acute onset of one or more
symptoms of dysuria, hematuria, frequency, urgency, urinary retention,
suprapubic pain, flank pain, or rigors that have positive urine culture
(a growth of = 105 colony forming units per mL).
A midstream urine culture and blood cultures
were obtained from each patient on day 2 after the biopsy and repeated
on day 14 after the biopsy. Patients recorded oral body temperature twice
daily for 2 weeks. Patients were asked to return for a follow-up visit
14 days after the biopsy. They were also advised to return immediately
if they had any complication, such as a high fever, chills.
Primary end-point of the study was to determine
the effect of needle guide on the bUTI rate. Secondary end point was sUTI.
Clinical symptoms and signs of infection were monitored weekly by office
interview.
Complications necessitating hospitalization
during the 2 week post-biopsy period were defined as serious. Statistical
analysis was performed using the Statistical Package for Social Sciences
(SPSS) for Windows Version 13.0 software (SPSS, Inc, Chicago, IL, USA).
Mean ages, serum total PSA levels, total prostate volume, comorbidities,
CRP and WBC in the groups were compared using univariate analysis of variance
test. Chi-squared test was used to compare infectious complication rates
between the groups. A p value less than 0.05 was considered significant
with a 95% confidence interval.
RESULTS
There were no significant differences between the two groups before the TPNB with respect to PSA levels, co-morbidities, CRP levels, and WBC counts. The data for each group is summarized in Table-1. The infectious complications are presented in Table-2. Bacteriologic UTI was observed in 3 patients (1 in Group 1 and 2 in Group 2). A total of 2 patients had Escherichia Coli (E. Coli) in blood culture (1 in each Group) and CRP levels were four times higher than before the TPNB in both groups. Two patients (1 in each Group) with high fever were admitted to the hospital and received intravenous antibiotic therapy. After receiving intravenous antibiotic therapy, the high fever and elevated CRP levels were controlled within 48 hours. E. Coli was harvested in urine culture in 1 patient in Group 2. This patient required hospitalization due to extended-spectrum beta-lactamase (ESBL) producing E. Coli harvested in urine culture in Group 2. No elevated CRP level or any signs of infection were recorded in this patient. Symptomatic UTI was diagnosed in 2 patients (1 patient in each group) caused by E. coli and received oral antibiotic therapy. All isolates were cipro?oxacin resistant. Bacteriologic and symptomatic UTI was detected in 4% vs. 6.6% and 4% vs. 3.9% in Group 1 and 2 respectively (p > 0.05).
COMMENTS
The
use of needle guide for TPNB reduces technique variability; leading to
a shorter learning curve for biopsy procedure; reduction in procedure
time; and a consistent replicable procedure (9). However, the risk of
cross-contamination is questionable. The disposable needle guide was introduced
into the market in an effort to reduce the risk of infection.
The clinical infection rates after TRNP
vary between 0.25 and 5% in past series, though other authors have reported
rates of up to 7.5% (10,11). After biopsy incidence of bacteremia and
bacteriuria were reported as 15% to 73% and 30% to 53% respectively (12,13).
Lindert et al. reported that bacteremia and bacteriuria after TPNB are
common but usually asymptomatic (4). Urine cultures alone may not be useful
for diagnosing infection (14). There is no unifying definition of infectious
complications after TPNB. However, bacteriologic investigation (bacteriuria
[more than 105 CFU/mL] versus no bacteriuria and bacteremia) and clinical
diagnosis (no clinical symptoms of UTI versus clinical signs of UTI) at
follow-up are determinant factors to evaluate the complications after
TPNB. The clinical importance of positive urine culture in asymptomatic
patients is unclear but one asymptomatic patient in group 2 required hospitalization
due to ESBL producing E. Coli harvested in urine culture.
Bacteriologic UTI rate was found to be statistically
similar in both groups. (4% vs. 6.6%).
Hospitalization was required in 4%, 6.6%
in Group 1 and Group 2 relatively. The failures of quinolone prophylaxis
might be the reason. Worldwide, quinolone-resistance rates among gram-negative
bacilli are rising rapidly. Turkish Urinary
Tract Infection Study Group recommended that fluoroquinolone-sparing agents
should be evaluated as alternative therapies by further clinical efficacy
and safety studies (15). Ozden et al. reported the high incidence of ESBL
producing E Coli after TRNP (16). New preventive protocols might be necessary
for TPNB.
Obek et al. reported periprostatic lidocaine
infiltration may be associated with a higher risk for infection due to
the extra 2 punctures of lidocaine injection into the periprostatic area
through the rectum, which is known to be highly colonized by bacteria
(17). Intracapsular punctures during anesthesia can also contribute to
the increased rate of infection after biopsy but both groups received
the same type of periprostatic anesthesia in this study.
There are many factors that are related to the risk of infectious complications
in prostate biopsies, such as lack of standardization among urologists
in pre-biopsy antimicrobial prophylaxis, high incidence of resistant organisms,
and the different methods of disinfection for reusable guides. Contamination
of the tools used in biopsies has been reported to be the possible cause
of infections occurring after TRUS-guided prostate biopsies (18). These
devices have a needle guide that directs biopsy needle insertion. The
biopsy needle repeatedly traverses the guide, affording the opportunity
for fecal and blood materials to accumulate. Bioburdens can also accumulate
in other parts of the transducer assembly. Brushes are required to clean
the transducer assemblies to reduce the bioburden and remove proteins.
Transducer assembly kits have not always been supplied with brushes. Not
using brushes for cleaning has resulted in improperly reprocessed transducer
assemblies, which could lead to pathogen transmission between patients.
Gillespie et al. (5) detected an outbreak of Pseudomonas aeruginosa after
prostate biopsy due to the insufficient manual cleaning of reusable needle
guides. They concluded that clinicians performing TRUS-guided prostate
biopsy procedures should follow the manufacturer’s needle guide
reprocessing recommendations or use disposable needle guides. In this
study we used the Toshiba Fabio reusable needle guide. According to our
results, all types of infectious complications such as asymptomatic bacteriuria,
acute urinary infection, high fever, and bacteremia occurred at a statistically
similar rate in both groups.
The permanent reusable needle guide, which
has a long, narrow lumen may not have allowed adequate sterilization,
as mentioned in previous studies, and may be the basis for the increased
risk of infectious complications. It is essential to review the manufacturer’s
reprocessing recommendations and to establish appropriate procedures to
avoid potential transmission of pathogens and subsequent patient concerns.
Potential sterilization problems with prostate biopsy equipment encourage
the use of disposable equipment. Tuncel et al. (8) first reported that
the use of a disposable needle guide reduces infectious complications.
These authors determined that asymptomatic bacteriuria, high fever, and
acute UTIs were statistically lower in the disposable group compared to
the reusable group a 4.5% vs. 9%; 5% vs. 10%; and 2% vs. 9%, respectively).
Inadequate flushing of the lumen with disinfectant to eradicate microorganisms
and the lack of availability of a device to clean the long, narrow lumen
was suggested as the major problem with the use of a reusable needle guide
for infectious complications. They concluded that the novel device which
has been used as a disposable needle guide is a good alternative to reduce
infectious complications. Our results are inconsistent with the results
of the initial study but our study population was smaller than previous
study populations, possibly affecting the power of our study. However,
if the infectious complications occur due to the contamination of the
needle guide, it may also occur due to the multiple reintroduction of
the needle during the same biopsy. Using a reusable needle guide, even
if the needle guide is changed after each pass of the needle, would provide
little difference versus a disposable guide. The other explanation is
that the physical features of the reusable needle guide in this study
may have allowed proper sterilization. The separable and detachable features
of the needle guide may be an important factor to prevent the possible
infections. The permanent type of reusable needle guide which has been
used in Tuncel et al. study (personal info from the author) might not
have allowed the appropriate cleaning.
The core sampling notch was approximately
17 mm long by 1.2 mm in diameter. The procedure time including anesthesia
application was 15 minutes for each case. There were no major technical
problems during the procedure. However,
the core length and the procedure time or some minor technical problems
may individually affect the infection rate. We did not focus on this issue.
In our study, there were no statistically
significant differences between the two groups regarding co-morbidity.
Therefore, it is difficult to conclude that the risk of infection is less
when using a disposable needle guide in patients with additional co-morbidities.
Although the number of patients was limited in our study; a reusable needle
guide was found to be safe in patients who had additional co-morbidities.
Reprocessing instructions for transrectal
biopsy equipment, such as a transducer, biopsy channel bracket, and needle
guide, is well-defined in the Food and Drug Administration recommendations
(19). The risks of transmission of hepatitis B virus, hepatitis C virus,
human immunodeficiency virus, during prostate biopsies were evaluated
by Lessa et al. (20). Although, on aggregate, their findings do not provide
evidence of disease transmission, although they do not rule out transmission
in some cases. We did not focus on viral transmission in this study. The
needle guide can be effectively disinfected with glutaraldehyde, but it
must be disassembled from the transducer assembly before disinfection.
We suggest that following the manufacturer’s guidelines for the
sterilization may be sufficient for using reusable instruments. The advantages
of using a disposable needle guide are that it does not need to be reprocessed
and it saves time, however, its cost is US$ 5.00 per patient. Since the
rate of infection appears to be same, whatever needle guide used, the
issue of cost bene?t ratio must always be kept in mind.
CONCLUSION
It seems to be ineffective to reduce the infection rate after the prostate biopsy by using a disposable needle guide. Large scale and randomized studies are necessary to determine the effect of disposable needle guide on infection rate after TPNB.
ACKNOWLEDGEMENTS
Mr. Rusen Celikoglu helped in this study.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Isen K, Küpeli B, Sinik Z, Sözen S, Bozkirli I: Antibiotic prophylaxis for transrectal biopsy of the prostate: a prospective randomized study of the prophylactic use of single dose oral fluoroquinolone versus trimethoprim-sulfamethoxazole. Int Urol Nephrol. 1999; 31: 491-5.
- Raaijmakers R, Kirkels WJ, Roobol MJ, Wildhagen MF, Schrder FH: Complication rates and risk factors of 5802 transrectal ultrasound-guided sextant biopsies of the prostate within a population-based screening program. Urology. 2002; 60: 826-30.
- Aron M, Rajeev TP, Gupta NP: Antibiotic prophylaxis for transrectal needle biopsy of the prostate: a randomized controlled study. BJU Int. 2000; 85: 682-5.
- Lindert KA, Kabalin JN, Terris MK: Bacteremia and bacteriuria after transrectal ultrasound guided prostate biopsy. J Urol. 2000; 164: 76-80.
- Gillespie JL, Arnold KE, Noble-Wang J, Jensen B, Arduino M, Hageman J, et al.: Outbreak of Pseudomonas aeruginosa infections after transrectal ultrasound-guided prostate biopsy. Urology. 2007; 69: 912-4.
- Huang YC, Ho DR, Wu CF, Shee JJ, Lin WY, Chen CS: Modified bowel preparation to reduce infection after prostate biopsy. Chang Gung Med J. 2006; 29: 395-400.
- Berger AP, Gozzi C, Steiner H, Frauscher F, Varkarakis J, Rogatsch H, et al.: Complication rate of transrectal ultrasound guided prostate biopsy: a comparison among 3 protocols with 6, 10 and 15 cores. J Urol. 2004; 171: 1478-80; discussion 1480-1.
- Tuncel A, Aslan Y, Sezgin T, Aydin O, Tekdogan U, Atan A: Does disposable needle guide minimize infectious complications after transrectal prostate needle biopsy? Urology. 2008; 71: 1024-7; discussion 1027-8.
- Phal PM, Brooks DM, Wolfe R: Sonographically guided biopsy of focal lesions: a comparison of freehand and probe-guided techniques using a phantom. AJR Am J Roentgenol. 2005; 184: 1652-6.
- Griffith BC, Morey AF, Ali-Khan MM, Canby-Hagino E, Foley JP, Rozanski TA: Single dose levofloxacin prophylaxis for prostate biopsy in patients at low risk. J Urol. 2002; 168: 1021-3.
- Peyromaure M, Ravery V, Messas A, Toublanc M, Boccon-Gibod L, Boccon-Gibod L: Pain and morbidity of an extensive prostate 10-biopsy protocol: a prospective study in 289 patients. J Urol. 2002; 167: 218-21.
- Petteffi L, Toniazzo GP, Sander GB, Stein AC, Koff WJ: Efficiency of short and long term antimicrobial therapy in transrectal ultrasound-guided prostate biopsies. Int Braz J Urol. 2002; 28: 526-32.
- Ruebush TK 2nd, McConville JH, Calia FM: A double-blind study of trimethoprim-sulfamethoxazole prophylaxis in patients having transrectal needle biopsy of the prostate. J Urol. 1979; 122: 492-4.
- Zegarra Montes LZ, Sanchez Mejia AA, Loza Munarriz CA, Gutierrez EC: Semen and urine culture in the diagnosis of chronic bacterial prostatitis. Int Braz J Urol. 2008; 34: 30-7, discussion 38-40.
- Yagci D, Yoruk F, Azap A, Memikoglu O: Prevalence and risk factors for selection of quinolone-resistant Escherichia coli strains in fecal flora of patients receiving quinolone therapy. Antimicrob Agents Chemother. 2009; 53: 1287-9.
- Ozden E, Bostanci Y, Yakupoglu KY, Akdeniz E, Yilmaz AF, Tulek N, et al.: Incidence of acute prostatitis caused by extended-spectrum beta-lactamase-producing Escherichia coli after transrectal prostate biopsy. Urology. 2009; 74: 119-23.
- Obek C, Onal B, Ozkan B, Onder AU, Yalçin V, Solok V: Is periprostatic local anesthesia for transrectal ultrasound guided prostate biopsy associated with increased infectious or hemorrhagic complications? A prospective randomized trial. J Urol. 2002; 168: 558-61.
- Centers for Disease Control and Prevention (CDC): Pseudomonas aeruginosa infections associated with transrectal ultrasound-guided prostate biopsies--Georgia, 2005. MMWR Morb Mortal Wkly Rep. 2006; 55: 776-7. Erratum in: MMWR Morb Mortal Wkly Rep. 2006; 55: 1177.
- US Food and Drug Administration. FDA public health notification; Reprocessing of Reusable Ultrasound Transducer Assemblies Used for Biopsy Procedures. 2006. Available at http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/PublicHealthNotifications/UCM062086
- Lessa F, Tak S, Devader SR, Goswami R, Anderson M, Williams I, et al.: Risk of infections associated with improperly reprocessed transrectal ultrasound-guided prostate biopsy equipment. Infect Control Hosp Epidemiol. 2008; 29: 289-93.
____________________
Accepted after revision:
July 30, 2010
_______________________
Correspondence address:
Dr. Cenk Gurbuz
2222 Medical District Dr. 4339
Dallas, TX 75235, USA
Fax: + 1 46 9422-9910
E-mail: gurbuzcenk@yahoo.com
EDITORIAL COMMENT
Transrectal
guided prostate needle biopsy (TPNB) is one of the most common outpatient
diagnostic procedures in urology clinics and in this study the authors
analyzed whether the use of disposable needle guide decrease the infectious
complication after TPNB. Fever after prostate biopsy was developed in
3.5% patients (1). Urosepsis and bacteremia were rare but bothersome complications.
Antibiotic prophylaxis including ciprofloxacin therapy has been administrated
in most of the urology clinics to prevent infectious complications. Recently,
Tuncel et al. suggested that the use of disposable needle guide could
reduce the infection risk after prostate biopsy (2). However, in the current
study the authors showed that it is ineffective to prevent infection.
Rutala et al. demonstrated that probe disinfection with glutaraldehyde
greater than 2% concentration could be achieved when prostate needle guide
was removed (3). Therefore, adequate cleaning and disinfection could explain
the similar infection risks of use disposable and reusable needle guide.
However, the small number of patients included in the study group prevents
definite clinical judgment.
In spite of these controversially results, the disposable needle guide
with a price of $5.00 should be used for biopsy to overcome the difficulty
in standardization of proper disinfection procedures in urology clinics.
Whenever disposable needle is not available, mechanical cleaning to remove
biologic material followed by 20 minutes of disinfection with glutaraldehyde
should be performed after removing the reusable needle guide.
REFERENCES
- Raaijmakers R, Kirkels WJ, Roobol MJ, Wildhagen MF, Schrder FH: Complication rates and risk factors of 5802 transrectal ultrasound-guided sextant biopsies of the prostate within a population-based screening program. Urology. 2002; 60: 826-30.
- Tuncel A, Aslan Y, Sezgin T, Aydin O, Tekdogan U, Atan A: Does disposable needle guide minimize infectious complications after transrectal prostate needle biopsy? Urology. 2008; 71: 1024-7; discussion 1027-8.
- Rutala WA, Gergen MF, Weber DJ: Disinfection of a probe used in ultrasound-guided prostate biopsy. Infect Control Hosp Epidemiol. 2007; 28: 916-9.
Dr.
Onur Kaygýsýz
Yalova State Hospital
Department of Urology
Yalova, TURKEY
E-mail: onurkygsz@yahoo.com
EDITORIAL COMMENT
The authors
should be commended on such a novel concept to potentially reduce infection
after transrectal prostate needle biopsy. The methodology used to detect
presence of infection was comprehensive and well designed. The randomized
cohorts did not demonstrate a significant difference with regard to infection
rates as a function of disposable versus reusable needle guide. The bacteriologic
infection rate was 4% in both groups while surprisingly, the symptomatic
urinary tract infection rate was greater for the disposable needle guide.
Infection rates after transrectal biopsy are not negligible and certainly,
any effort to reduce them should be explored. Our group has offered stereotactic
transperineal prostate biopsy (STPB) for patients that have had prior
negative transrectal prostate biopsy despite continued elevation of PSA
(1,2). While 40% of these patients are identified as having occult malignancy
after STPB, an additional benefit has been a true null of post procedure
infection. I acknowledge that STPB is not widely accepted as a first line
biopsy technique, but given the high diagnostic yield and negligible risk
of infection, STPB may be more commonplace in the future.
REFERENCES
- Moran BJ, Braccioforte MH: Stereotactic transperineal prostate biopsy. Urology. 2009; 73: 386-8.
- Moran BJ, Braccioforte MH, Conterato DJ: Re-biopsy of the prostate using a stereotactic transperineal technique. J Urol. 2006; 176: 1376-81; discussion 1381.
Dr.
Brian J. Moran
Chicago Prostate Cancer Center
Westmont, Illinois, USA
E-mail: seeds@prostateimplant.com