IMAGING IN URINARY TRACT OBSTRUCTION
CAROLINE D. AMES, ROBERT A. OLDER
Departments of Urology and Radiology, University of Virginia Health System, Charlottesville, Virginia, USA
ABSTRACT
There
are a wide variety of imaging studies available for evaluation of a potentially
obstructed patient. Selection of a specific test over another depends
on the acuity of obstruction and the patient’s age and renal function.
Consideration must also be made for cost of the test, reliability and
feasibility of long term follow up by repeated exams. In the non-acute
setting where urinary tract obstruction is suspected either on the basis
of a rising serum creatinine, history, or prior urinary tract abnormalities,
an ultrasound may be used as the initial screening procedure. If ultrasound
fails to show any evidence of significant hydronephrosis or hydroureter
it is concluded that this patient does not have significant obstruction.
Generally, no further studies relative to detecting urinary tract obstruction
are performed.
If ultrasound demonstrates the presence
of hydronephrosis or hydroureter further studies to determine the point
and cause of obstruction are performed, unless the ultrasound examination
has clearly demonstrated this, as in the case of an obstructing ureteral
stone. In adults, an intravenous pyelography (IVP) is often perform to
delineate the point and hopefully cause of an obstruction. If there is
good renal function, the IVP will generally be successful in answering
these questions. There is not always one “best” way to utilize
the multiple studies available and it is often the results of a specific
study that will determine if a further study is necessary and which modality
to use.
The approach to the patient with acute renal
colic has changed over the past few years. Up until recently, these patients
were evaluated with either ultrasound or an IVP as the initial study.
This is no longer the case as we now use non-contrast spiral computed
tomography (CT) as the screening examination for flank pain and suspected
ureteral stone. This is faster, more accurate and provides information
regarding non-urologic causes of pain.
In children, the approach is somewhat different.
Ultrasound is used as the primary screening tool for suspected obstruction.
If hydronephrosis is demonstrated, a functional study such as a Lasix
renogram is generally performed to evaluate the function of the two kidneys
and the severity of the suspected obstruction. Further study would then
depend on clinical consideration such as any need for surgical intervention.
Key words:
urinary tract; obstruction; imaging; kidney; ureter; calculi
Braz J Urol, 27: 316-325, 200
IMAGING IN OBSTRUCTION
There are numerous studies available to the urologist in the diagnosis and management of obstruction. These include radiographic studies, such as the plain film (kidney, ureter and bladder – KUB), intravenous pyelography (IVP) and retrograde urography, ultrasound, computed tomography (CT), Lasix renogram, magnetic resonance (MR) urogram and the Whitaker test. Selection of a specific test over another depends on the acuity of obstruction and the patient’s age and renal function. Pregnant patients and those with contrast allergy require special provisions. Consideration must also be made for cost of the test, reliability and feasibility of long term follow up by repeated exams. We will explore each imaging modality listed and then discuss our approach to the patient with suspected obstruction.
PLAIN FILM
Simple
radiographic studies such as the KUB have a role, although limited, in
the evaluation of obstruction. A single view plain film may be sufficient
to diagnose the presence of a ureteral stone. It is low cost with low
radiation exposure and may be done rapidly within the urology clinic.
The plain film is limited by its low sensitivity for detection of opaque
as well as non-opaque stones. Recent studies have shown a sensitivity
of about 50% for stone visualization with the abdominal film. Occasionally
a suspected ureteral calcification seen on plain film turns out to be
a vascular phlebolith when more specific studies are performed (1).
The plain film also provides an easy way
to follow the progression of an obstructing stone, even if the diagnosis
of stone disease has been made with another imaging modality such as CT
scan. Significantly, more stones can be seen on an abdominal film in retrospect
following CT (2). Stones larger than 5 mm and with CT attenuation above
300H will likely be detected on abdominal radiography (3).
INTRAVENOUS PYELOGRAPHY
Intravenous
pyelography (IVP) plays an important role in the diagnosis of obstruction.
It is the classic test which can assess anatomy and to some extent the
function of the kidney. Acute obstruction is identified by the presence
of a delayed and often increased nephrogram (Figure-1). Hydronephrosis
or hydroureter helps to confirm the diagnosis of obstruction, but are
not always visible (1). The level and cause of the obstruction may be
determined with the visualization of filling defects or stones (Figure-2)
in the renal pelvis or ureter, changes in renal contour and course of
the ureters. In addition, bladder pathology may be revealed on IVP, such
as filling defects, diverticula and a significant post void residual.
Obstructions, which are not obvious initially, may, at times, be revealed
after the administration of Lasix during the IVP. This technique is generally
reserved for suspected intermittent ureteropelvic junction (UPJ) obstruction.


The IVP requires intravenous contrast and
therefore should not be performed in a patient with decreased renal function.
We accept creatinine values of 1.5 or lower for patients undergoing IVP
in our department. Nephrotoxicity of iodinated contrast is most likely
in patients with chronic renal insufficiency especially if diabetes is
also present. Patients with contrast allergy need to be premedicated prior
to an IVP and should have non-ionic contrast media. The need for the IVP
must be balanced against potential risks. It may be wiser to perform alternate
studies in certain situations, such as a noncontrast CT scan, ultrasound
or magnetic resonance imaging (MRI). The availability of multiple other
modalities not requiring contrast has reduced dependence on the IVP. IVP
may be time intensive, requiring delayed films in patients with high-grade
obstruction and may not always have sufficient opacification to define
the anatomy and point of obstruction. In addition, completion of an IVP
requires a significant amount of radiation exposure and may not be ideal
for young children or pregnant women (1).
RETROGRADE UROGRAPHY
Retrograde urography, although largely replaced by other imaging studies, can still be useful to delineate the precise location and severity of an obstruction when other studies fail to define the exact point or cause of obstruction. In addition, this study can usually be performed with greater safety in patients who are not candidates for an IVP due to an allergy to contrast media or renal insufficiency. This is not a first line study for patients with obstruction due to the necessity of anesthesia, either general or epidural blockade. However, we often perform retrogrades in the operating room just prior to pyeloplasty or ureteral stent placement to exactly delineate the point of obstruction and to rule out the presence of a second obstruction.
ULTRASOUND
Ultrasound
is used extensively to detect hydronephrosis, the primary finding with
an obstructed system. It is inexpensive, noninvasive and portable.
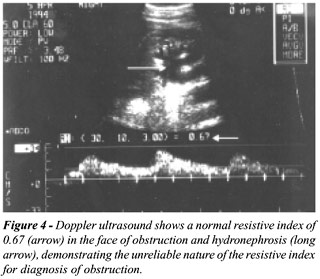
Ultrasound is an ideal first line technique
to evaluate patients for renal obstruction. It is highly sensitive in
detecting dilated systems (Figure-3) and the absence of hydronephrosis
is generally a reliable sign that obstruction is not present. An exception
is very early obstruction, such as might occur with an acute obstructing
stone. Resistive index has been advocated to detect these cases of early
obstruction (4) and is occasionally used in our clinic but has not proven
to be reliable (Figure-4) (5,6).

Because not all dilated systems represent
functional obstruction, ultrasound is therefore not specific. The imaging
findings must be correlated with the clinical picture. Hydronephrosis
not due to obstruction can result from prior obstruction, reflux, enlarged
extra renal pelvis, bladder over distension or a distensible collecting
system in a well hydrated individual. Renal sinus cysts may be mistaken
for a dilated renal pelvis on ultrasound, and a skilled ultrasonographer
is needed to make this differentiation.
Ultrasound is very accurate in the identification
of renal stones that may or may not be visible on plain radiograph, due
to either stone composition or size. However, detection of ureteral stones
by ultrasound is much more difficult. These stones often go undetected
by ultrasound unless they are near the ureteral tunnel (Figure-5). The
technical difficulties in detecting stones, operator dependence and relatively
low sensitivity for ureteral stone detection with ultrasound have led
to widespread shift to non-contrast spiral CT to evaluate renal colic
and suspected acutely obstructing stones.

Prenatal ultrasound is performed routinely
and may pick up evidence of hydronephrosis in the developing fetus. In
patients diagnosed with prenatal hydronephrosis, ultrasound should be
repeated within several weeks of birth to evaluate for persistent hydronephrosis
(7).
Because ultrasound is readily available
within our clinic, we use it to monitor patients with known obstruction.
A caveat to heavy reliance on ultrasound is that ultrasound is extremely
operator-dependent. It is ideally performed by personnel experienced in
uro-ultrasonography.
The ultrasonographer may also use color Doppler to evaluate the presence
of ureteral jets. The periodic “jet” of urine effluxing from
the ureteral orifice effectively rules out complete obstruction of the
renal system (1,8).
COMPUTED TOMOGRAPHY
Computed
Tomography (CT) scans can be performed with or without intravenous contrast.
Spiral CT scans use 5 mm slices from the level of the kidneys down to
the bladder specifically to look for stone disease. It has been shown
that the “stone-protocol” CT scan is more effective in precisely
identifying ureteral stones than the long time gold standard, the IVP
(9,10). CT is ideally suited to detecting obstructing stones and is very
effective in distinguishing the stone from other causes of obstruction
such as clot or tumor (1). Spiral CT scans may pick up stones that cannot
be seen on plain film (KUB) due to stone composition, size or artifacts
such as bowel gas. It is also useful to differentiate between calcifications
within the vascular system versus the urinary system.
CT diagnosis of a ureteral stone relies
on both primary and secondary findings. The primary finding is unequivocal
demonstration of a stone within the ureter (Figure-6). Secondary findings,
which include hydronephrosis, hydroureter or stranding of the perinephric
fat, have a high positive and negative predictive value for the presence
or absence of a ureteral stone (Figure-7) (1,11). Perinephric edema has
been showed to be predictive of the degree of obstruction (12). However,
it should be noted that non-contrasted CT scans could miss other causes
of flank pain and hematuria, such as a solid renal mass. It has been suggested
that patients with the diagnosis of a suspected ureteral stone that is
not seen on CT be followed by a contrasted CT to rule out other diagnoses
(13). Potential causes of extrinsic obstruction such as malignancy or
aneurysm may also be identified on CT scan (1), (Figure-8). During a dynamic
enhanced CT scan, a sign of obstruction is a delay in the nephrogram with
persistence of corticomedullar differentiation as compared to the opposite
kidney (Figure-8). Although CT picks up most stones, including those that
are classically opaque on plain film, it may miss obstruction caused by
non-opaque indinavir crystals. In patients with HIV on the protease inhibitor,
indinavir, presenting with acute flank pain, the absence of a stone on
helical CT should be followed with a contrasted CT scan (14).



We occasionally use contrasted CT scans
following a spiral (non-contrasted) scan to help define the course of
a ureter if we are unsure if a calcification resides within a ureter or
a vessel. Contrasted CT scans will further assess function of a renal
unit and more accurately detail the degree of hydroureteronephrosis.
LASIX RENOGRAM
The
Lasix renogram is very useful in the diagnosis and follow up of children
with UPJ obstruction. It is crucial in the identification of an obstructed
hydronephrotic kidney versus a non-obstructed hydronephrotic kidney. Previously,
it was assumed that any dilatation of an upper urinary system equaled
obstruction. We now know that a hydronephrotic kidney may simply represent
a dysmorphic or atonic collecting system, which has no functional significance
and will not cause renal damage over time. Therefore, all children with
suspected UPJ obstruction at our institution undergo diuretic renal scan
to determine the functional significance of hydronephrosis. A radionuclide
is administered and then the scintillation camera obtains individual counts
from each kidney, which are then expressed as a percent of the total.
We use 99mTc-MAG3, which collects in the collecting system due to tubular
secretion and has good uptake in patients with renal insufficiency (1).
Diuretics are used as a part of the renogram in order to separate non-obstructive
hydronephrosis from obstructive hydronephrosis. A diuretic is given after
the radionuclide has accumulated in the collecting system. Then the “washout
time” of the radionuclide is determined. In the absence of obstruction,
the diuretic will fill the collecting system with urine not containing
the radionuclide and the urine that contains radionuclide will be washed
out of the system. However, in the presence of obstruction, the radionuclide
is not washed out as quickly. The T½ is a value measured as the
time it takes for 50% of the tracer to leave the collecting system. This
clearance half-time is based on the slope of the washout curve. A T½
of less than 15 minutes is normal. In general, a T½ of greater
than 20 minutes represents obstruction. (Figure-9) (15). In addition to
the T½, the Lasix renal scan will also allow estimation of the
split renal function. Split function allows the clinician to closely monitor
renal function in patients managed conservatively and in postoperative
studies (15).

Although the Lasix renogram can supply very
useful information, urologists should keep in mind that there are several
factors which can make the results unreliable. First of all, poor renal
function may cause an inability to respond to the diuretic, resulting
in a false delay in washout time. Poor hydration may also limit the response
to diuretic (15). Secondly, there is no standard protocol for the administration
or the interpretation of the Lasix renogram. Care should be taken when
comparing studies performed in two different institutions (16). It is
crucial that a standard protocol be developed and maintained at all times
within a single center to facilitate comparison of scans over time. At
the University of Virginia, we follow the protocol outlined by Conway
(17) in an effort to standardize the protocol of performing a Lasix renogram.
His guidelines include:
a)- Oral hydration;
b)- Bladder catheterization in any patient who cannot void on request;
c)- Patient at least 1 month old;
d)- Use of a standard radionuclide-99mTc-MAG3;
e)- Diuretic given at 1mg/kg when the abnormal collecting system is full.
Finally, the diuretic renogram identifies
the presence of obstruction but not the cause of obstruction. There is
very little anatomic detail provided with the Lasix renogram (1,18).
MAGNETIC RESONANCE UROGRAM
Magnetic
resonance imaging provides more detailed anatomy than nuclear renograms
without the radiation exposure or the use of potentially nephrotoxic contrast
media, which is necessary for IVP. We occasionally employ the MR urogram
(MRU) with gadolinium to replace the IVP in a patient with renal insufficiency
or contrast allergy or in a patient population that requires reduced radiation
exposure (i.e., pregnant women). The MR urogram delineates the presence
and degree of hydronephrosis and may pick up filling defects within the
collecting system (Figure-10). In a patient with poor renal function,
MRU may provide more detailed anatomy than IVP. MR urography has not become
popular at most institutions due to several shortcomings. Although there
is good resolution of the renal parenchyma and the collecting system,
the anatomy of the calices is not seen with optimal detail, as in an IVP.
This may miss a diagnosis of papillary necrosis. The diagnosis of a small
ureteral stone may also be missed on MRU (19). Patients who are severely
claustrophobic or require close hemodynamic monitoring or who are unable
to cooperate may be inappropriate for MR. Patients with cardiac pacemakers,
cochlear implants, brain aneurysm clips or prosthetic heart valves are
not candidates for MR. Finally, MR is limited due to cost and availability
(20,21).

WHITAKER TEST
The
Whitaker test, a ureteral pressure-flow study, provides a precise but
invasive measure of the presence or absence of obstruction in the face
of hydronephrosis. It allows direct measurement of ureteral resistance
by recording the pressure gradient across the suspected area of obstruction.
Results delineate the functional significance of the obstruction. Performance
of the Whitaker test requires placement of a catheter in the bladder as
well as an antegrade pyelogram needle in the kidney. Contrast is delivered
at a constant rate through the needle in the kidney, simulating diuresis,
and pressures in the kidney and the bladder are measured. Inaccuracy may
be encountered in the face of variable renal anatomy or compliance. Furthermore,
the Whitaker test assumes that the obstruction is constant over time,
which may produce false negative results (22).
The presence of hydronephrosis does not,
in and of itself, imply obstruction. Other causes of hydronephrosis may
include: high output by the renal unit, permanent dilation from an old
obstruction that has since resolved, vesicoureteral reflux, calyceal dilation
of congenital megacalycosis or papillary necrosis, or an extra renal pelvis
(23). It is important to document the presence of functional obstruction
before any intervention is planned.
URETEROPELVIC JUNCTION
OBSTRUCTION
Ureteropelvic
junction obstructions may be classified as either chronic or acute. The
majority are chronic and congenital in origin although they may not become
clinically apparent until childhood or even adulthood (24). Frequently,
pathology of the obstructed segment reveals an aperistaltic ureteral segment
in which the normal spiral musculature has been replaced by abnormal fibrous
tissue and longitudinal muscle bands. Other causes of chronic UPJ obstruction
include congenital stricture, kinks or valves within the ureter caused
by infoldings of the mucosa, angulation of the ureteral insertion on the
pelvis and aberrant vessels entering directly into the lower pole of the
kidney causing external compression of the ureter (22,25).
Acquired causes of chronic UPJ obstruction
include vesicoureteral reflux which causes upper tract dilation and tortuosity
of the ureter, benign fibroepithelial polyps, transitional cell carcinoma,
post operative or post inflammatory scarring and stones (22).
UPJ obstruction is suspected in neonates
and infants presenting with a palpable flank mass or hydronephrosis on
prenatal ultrasound. Older children and adults may present with flank
or abdominal pain that may be intermittent in nature. Alternatively, they
may present with urinary tract infections or microscopic hematuria. The
diagnosis is confirmed with ultrasound (Figure-9).
In chronic UPJ obstruction, there may be
significant loss of renal function before the diagnosis is made. Studies
should be performed to consider the amount of renal function still present
and how much is salvageable. Lasix renogram studies with split function
analysis are crucial for adding this information. Before operative intervention
such as pyeloplasty is performed, retrograde urograms may be obtained
to delineate the exact site of obstruction and to rule out a second, distal
obstruction. This is often done on the same day as the planned repair
in order to avoid the use of two general anesthetics.
APPROACH TO THE POTENTIALLY OBSTRUCTED PATIENT
There
are a wide variety of imaging studies available for evaluation of a potentially
obstructed patient. Our approach to this patient is determined by the
clinical setting. In the non-acute setting where urinary tract obstruction
is suspected either on the basis of a rising serum creatinine, history,
or prior urinary tract abnormalities we will use ultrasound as the initial
screening procedure. If ultrasound fails to show any evidence of significant
hydronephrosis or hydroureter it is concluded that this patient does not
have significant obstruction. Generally, no further studies relative to
detecting urinary tract obstruction are performed.
If ultrasound demonstrates the presence
of hydronephrosis or hydroureter further studies to determine the point
and cause of obstruction are performed, unless the ultrasound examination
has clearly demonstrated this, as in the case of an obstructing ureteral
stone. In adults, we will often perform an IVP to delineate the point
and hopefully cause of an obstruction. If there is good renal function,
the IVP will generally be successful in answering these questions. If
there is reduced renal function due to a long-standing obstruction, or
for other reasons, the IVP may not provide sufficient visualization of
the collecting structures to define the etiology of the obstruction. In
these instances retrograde pyelogram is performed which, if technically
successful, will usually define the point of obstruction. If the etiology
is intrinsic to the urinary tract further studies are generally not necessary.
If, however, the studies demonstrate what appears to be an extrinsic cause
of the obstruction, computed tomography, with contrast if possible, is
performed to look for evidence of mass lesions (Figure-8C) or fibrotic
change. There is not always one “best” way to utilize the multiple
studies available and it is often the results of a specific study that
will determine if a further study is necessary and which modality to use.
Although not used often at our institution, MRI urography can demonstrate
both intrinsic and extrinsic abnormalities related to the urinary tract
and is particularly helpful in those patients in whom contrast cannot
be used.
Our approach to the patient with acute renal
colic has changed over the past few years. Up until recently, these patients
were evaluated with either ultrasound or an IVP as the initial study.
This is no longer the case as we now use non-contrast spiral CT as the
screening examination for flank pain and suspected ureteral stone. This
is faster, more accurate and provides information regarding non-urologic
causes of pain. In most cases, the non-contrast study will determine the
presence and cause of obstruction, especially if due to a ureteral stone.
If an obstruction secondary to a ureteral stone is identified and the
stone is to be followed, we will often obtain an abdominal film for the
purposes of follow-up. Unfortunately, only approximately 70% of stones
detected on CT scanning will be demonstrable on an abdominal film even
in retrospect. If the obstructing stone cannot be identified on an abdominal
film and follow-up imaging is necessary because of the patient’s
clinical course then either a follow-up non-contrast spiral CT or in some
cases an IVP can be obtained to assess the persistence and degree of obstruction
as well as the position of the stone.
If the non-contrast spiral CT shows no evidence
of a ureteral stone but does show hydronephrosis or hydroureter, correlation
is made with clinical findings to determine if this may represent passage
of a stone prior to the CT scan. If this is the case, clinical follow-up
will determine further imaging. Otherwise, IVP will be performed to evaluate
for other causes of obstruction.
In children, our approach is somewhat different.
Ultrasound is used as the primary screening tool for suspected obstruction.
If hydronephrosis is demonstrated, a functional study such as a Lasix
renogram is generally performed to evaluate the function of the two kidneys
and the severity of the suspected obstruction. Further study would then
depend on clinical consideration such as any need for surgical intervention.
In summary, multiple techniques exist for
the evaluation of renal obstruction. Each patient must be evaluated on
an individual basis with consideration of the acuity of obstruction and
the special needs of the patient. Certain centers may not have access
to helical CT scanners, nuclear medicine capabilities or a MRI. Techniques
must be reliable and accessible to allow the clinician to follow the disease
over time.
REFERENCES
- 1. Keolliker SL, Cronan JJ: Acute urinary tract obstruction. Imaging update. Urol Clin North Am, 24: 571-582, 1997.
- Levine JA, Neitlicht, Vergan: Ureteral calculi in patients with flank pain: correlation of plain radiography with enhanced of plain radiography with unenhanced helical CT. Radiology, 204: 27-31, 1997.
- Zagoria RJ, Khatod EG, Chen MYM: Abdominal radiography after CT reveals urinary calculi: a method to predict usefulness of abdominal radiography on the basis of size and CT attenuation of calculi. AJR, 176:1117-1122, 2001.
- Platt JF, Rubin JM, Ellis JH: Acute renal obstruction: evaluation with intrarenal duplex Doppler and conventional US. Radiology, 186: 685, 1993.
- Tublin ME, Dodd GD III, Verdile VP: Acute renal colic: diagnosis with duplex Doppler US. Radiology, 193: 697, 1994.
- Older RA, Stoll HL, Omary RA, Watson LR: Clinical value of renovascular resistive index measurement in the diagnosis of acute obstructive uropathy. J Urol, 157: 2053-2055, 1997.
- Ebel KD: Uroradiology in the fetus and newborn: diagnosis and follow-up of congenital obstruction of the urinary tract. Pediatric Radiology, 28: 630-635, 1998.
- Cox IH, Erickson SJ, Foley WD, Dewire DM: Ureteric jets: evaluation of normal flow dynamics with color Doppler sonography. AJR, 158: 1051-1055, 1992.
- Smith RC: Acute flank pain: comparison of non-contrast-enhanced CT and intravenous urography. Radiology 194: 789-794, 1995.
- Niall O, Rusell J, MacGregor R: A comparison of noncontrast computerized tomography with excretory urography in the assessment of acute flank pain. J Urol, 161: 534-537, 1999.
- Zagoria RJ: Helical CT of urolithiasis: leaving no stone unturned. Appl Radiol, 10: 8-13, 1998.
- Boridy IC: Acute ureterolithiasis: Nonenhanced helical CT findings of perinephric edema for prediction of degree of ureteral obstruction. Radiology, 213: 663-667, 1999.
- Chong WK: Renal carcinoma presenting with flank pain: a potential drawback of unenhanced CT. AJR, 174: 667-669, 2000.
- Blake SP, McNicholas MM, Raptopoulos V: Nonopaque crystal deposition causing ureteric obstruction in patients with HIV undergoing indinavir therapy. AJR, 171: 717-720, 1998.
- Kass EJ, Fink-Bennet TD: Contemporary Techniques for the Radioisotopic Evaluation of dilated urinary tracts. Urol Clin North Am, 17: 273-289, 1990.
- Roarke MC, Sandler CM: Provocative imaging: diuretic renography. Urol Clin North Am, 25: 227-249, 1998.
- Conway JJ: “Well-tempered” diuresis renography: its historical development, physiological and technical pitfalls, and standardized technique protocol. Seminars in Nuclear Medicine, 22: 74-84, 1992.
- Dubovsky EV, Russell CD: Advances in radionuclide evaluation of urinary tract obstruction. Abdominal Imaging, 23:17-26, 1998.
- Hussain S: MR urography. Magnetic Resonance Imag Clin North Amer, 5: 95-106, 1997.
- Roy C: MR urography in the evaluation of urinary tract obstruction. Abd Imag, 23: 27-34, 1998.
- Dockery WD, Stolpen AH: State-of-the-art magnetic resonance imaging of the kidneys and upper urinary tract. J Endourol, 13: 417-423, 1999.
- Koff SA: Pathophysiology of ureteropelvic junction obstruction. Urol Clin North Am, 17: 263-272, 1990.
- Papanicolaou N: Urinary Tract Imaging and Intervention: Basic Principles. In: Walsh PC, Retik AB, Vaughan ED, Wein JA (eds.). Campbell’s Urology, Philadelphia, WB Saunders, pp. 243-244, 1998.
- Jacobs JA: Ureteropelvic obstruction in adults with previously normal pyelograms: a report of 5 cases. J Urol, 121: 242-244, 1979.
- Park JM, Bloom DA: The pathophysiology of UPJ obstruction: current concepts. Urol Clin North Am, 25:161-169, 1998.
____________________
Received: May 11, 2001
Accepted: May 30, 2001
_______________________
Correspondence address:
Dr. Robert A. Older
University of Virginia Health System
Department of Radiology
P.O. Box 800170
Charlottesville, VA 22908, USA
Fax: + + (1) (804) 982-4019
E-mail: rao2k@virginia.edu