SELECTIVE
SEROTONIN RE-UPTAKE INHIBITOR IN THE TREATMENT OF PREMATURE EJACULATION
(
Download pdf )
JOSÉ P.T. NOVARETTI, ANTONIO C.L. POMPEO, SAMI ARAP
Division of Urology, School of Medicine, University of São Paulo (USP), São Paulo, SP, Brazil
ABSTRACT
Introduction
and Objectives: This prospective, double-blind, randomized, cross-over,
placebo-controlled study was designed to investigate the efficacy and
side effects of the selective serotonin re-uptake inhibitors, fluoxetine
hydrochloride, on postponing ejaculation in patients with premature ejaculation
(PE).
Patients and Methods: A total of 55 men
with PE were scheduled to begin this study, but 5 dropped out. All patients
were heterosexual, ages 19 to 65 who experienced primary premature ejaculation
(lifelong rapid ejaculation). They were evaluated at the start and at
the end of the study to evaluate the degree of anxiety and depression
using the Hamilton Anxiety Scale and Beck et al. Partners were asked to
determine the time between vaginal penetration and ejaculation (latency
time), by using a clock marking the seconds. Treatment phases consisted
of an 8-week administration period of placebo or fluoxetine capsules,
4 weeks of wash-out and an additional 8-week cross-over treatment. All
patients were interviewed before and 8, 12 and 20 weeks after beginning
the treatment.
Results: Baseline mean ejaculatory latency
time was 60.6 s; 20 mg/day of fluoxetine increased it to 199.3 s (p <
0.001). This resulted in significantly greater sexual satisfaction for
men: 68% (p < 0.001). Generally, fluoxetine was well tolerated and
there were no major side effects. None of the patients discontinued therapy
due to adverse effects. No significant alterations in the Hamilton Anxiety
Scale and Beck et al. Scale for Depression scores at the beginning and
at the end of the study were observed. Anxiety and depression showed no
influence in the improvement of PE treated with Fluoxetina hydrochloride.
Conclusion: Fluoxetina hydrochloride may
be regarded as a safe and effective option in the treatment of premature
ejaculation.
Key words:
ejaculation; fluoxetine; antidepressant drugs; sexual dysfunction
Braz J Urol, 28: 116-122, 2002
INTRODUCTION
Premature
Ejaculation (PE) is the most common sexual dysfunction, which, according
to some authors (1), affects almost 50% of men. Because the ejaculation
occurs much sooner than desired, it causes a significant suffering for
the patient, as it impedes a satisfactory sexual intercourse.
There are many definitions of PE in the
medical literature; however, there is no consensus.
A quantitative definition is being formulated
to obtain parameters to be used in scientific studies. The most used parameter
has been the latency time, which is the time between vaginal penetration
and ejaculation.
However, there is not an agreement on how
long this time should be. Therefore, to Waldinger et al. (2), the patient
with PE ejaculates in less than a minute; to Strassberg et al. (3) in
less than two minutes; to Althof et al. (4), in less than four minutes
and to Schover et al. (5) in less than seven minutes.
Nowadays, the definition almost universally
accepted is the “DSM IV”, Mental Disorders Diagnostic and Statistical
Manual – 4th Edition, from the Psychiatric American Association,
published in 1994: “Premature Ejaculation is an ejaculation, persistent
or recurrent, with minimal sexual stimulation, before or thereupon ejaculation,
sooner than desired”. Occasional problems, not persistent and non-recurrent,
or not accompanied by great suffering or personal relationship difficulty,
do not characterize the diagnosis.
Many authors (6-11) have considered anxiety
the most important etiologic factor in the PE.
The non-drug treatment for PE has been traditionally
performed with behavioral therapies, using training, associated or not
to psycotherapy. This therapeutic modality demands very well-selected
patients and the results are generally not long lasting.
As from the sixties, it has been observed
that antidepressant, such as monoamine oxidase inhibitors (MAOIs), produce
side effects delaying or inhibiting ejaculation and orgasm (12).
As from the seventies, the use of serotonin
re-uptake inhibitors (clomipramine, fluoxetine, paroxetine and setraline)
on a large scale to treat depression, showed that they also affect ejaculation
significantly.
Clomipramine has been the most used one;
however, the side effects make its usage difficult in an expressive number
of cases (4,12,13).
The fluoxetin hydrochloride is an antidepressant
with strong action as selective serotonin re-uptake inhibitor, with few
or no effect on monoamines re-uptake. Therefore, it has a lower incidence
of side effects when compared to tricyclic antidepressants.
The objective of this study was to evaluate,
through a prospective, randomized, double-blind, cross-over, placebo-controlled
study, the efficacy of this drug in the treatment of PE and its side effects.
We also tried to evaluate the results in relation to anxiety and depression,
when present.
MATERIALS AND METHODS
One
hundred and eighty-three men were interviewed, without distinction of
color or race, with PE complaint for at least six months. Data were collected
from June 5th,1998 and January 7th, 2000.
One hundred and twenty-eight patients were
excluded: 48 had erectile dysfunction, 3 were using antidepressants, and
24 did not have a fixed partner or had irregular sexual intercourse. A
total of 53 patients did not return after the first interview. At the
end, 55 patients attended all inclusion criteria, but 5 abandoned the
study as soon as it started because of personal problems not-related to
the medication.
In the first appointment, after explaining
the study and giving the written consent, the patient was asked to return
after 4 weeks. During this period, the patient was asked to have at least
one intercourse per week, and to evaluate the time between penetration
and ejaculation. Time evaluation should be made by the partner with a
clock marking seconds.
Initial time was obtained through the arithmetic
mean of the four times measured. Besides the latency time obtained, a
subjective evaluation of the satisfaction level in relation to the sexual
intercourse was requested. Satisfaction level could vary from bad, fair
or good.
In the first appointment, the patient was
asked to answer 2 questionnaires: the Hamilton Anxiety Scale, to evaluate
the anxiety level, and Beck et al. Depression Scale, to evaluate the depresion
state.
Biographic data of all patients are summarized
in Table-1. All of them reported good affective relationship with their
partner and considered their sexual performance bad.

Patients were randomized in 2 groups: one
using 20 mg of fluoxetin a day, and the other using placebo, one tablet
a day, at 10 o’clock. The medication, identified by the letters A
or B, were provided by the pharmacological laboratory in identical tablets.
Boxes contained 56 tablets and the code (the letter corresponding to the
fluoxetin or the letter corresponding to the placebo), which was kept
in sealed envelope until the completion of data collection from all patients.
Both the researcher and the patients did not know who was taking the active
drug and who was taking the placebo (double-blind).
Patients started with the medication A or
B and returned 8 weeks later, when the first phase was over, bringing
the time of 8 sexual intercourse recorded. At the end of this period,
patients did not use the medication for 4 weeks (wash-out), and returned
bringing the time of 4 sexual intercourse recorded. After that, they started
to take the second medication (B or A), for more 8 weeks and returned
again with the duration of 8 sexual intercourse recorded.
The arithmetic mean of the latency time
measured, the satisfaction level with the sexual intercourse and the eventual
side effects were written in the protocol every time the patient returned.
In the last day, patients filled out once
again the Hamilton and the Beck et al. Scales to evaluate their anxiety
level and depression state. The results were compared to the ones initially
obtained.
The chosen fluoxetin dose was 20 mg once
a day, since this is the most common dose used in the treatment of anxiety
and depression, which causes ejaculation delay in many patients without
PE. This effect can be initiated in the first days of use. The four-week
period for wash out chosen was based on the fluoxetin half-life. The numerical
data obtained were described in mean, standard deviation and median.
The chi-square test, Fisher exact test,
Mann-Whitney test and Z test were used for the statistical analysis. We
adopted a significance level of 5% for all tests.
RESULTS
By
the end of the data collection period, the analysis of the 50 patients’
data provided results about many characteristics of patients with PE.
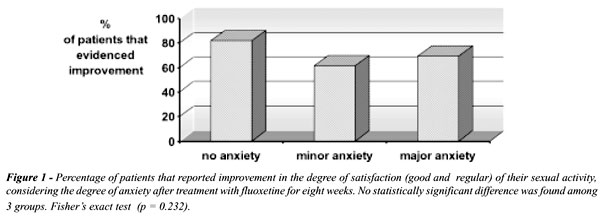
Using the data obtained from the Hamilton
Anxiety Scale and the Beck et al. Depression Scale, it was observed that,
in the beginning of the research, 11 patients had major anxiety, 26 minor
anxiety and 13 no anxiety (Table-2). Three patients had moderate depression,
9 light depression and 38 no depression (Table-3).
The questionnaires answered at the end of
the study reveled that no patient changed his anxiety level or depression.
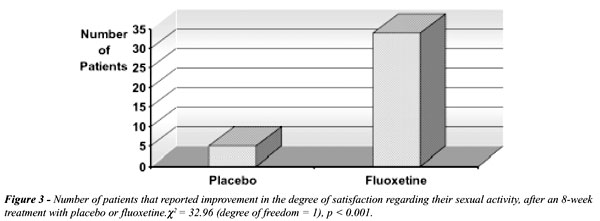
In relation to the satisfaction level with
sexual intercourse, the results showed that 27 patients (54%) reported
good improvement with fluoxetin, 7 (14%) reported fair improvement and
16 (32%) didn’t report any alteration, that is, they still had bad
quality sexual intercourse. During the placebo period, only 5 patients
(10%) reported fair improvement and 40 (90%) did not report improvement
(Table-4). The difference was statistically significant (p < 0.001).

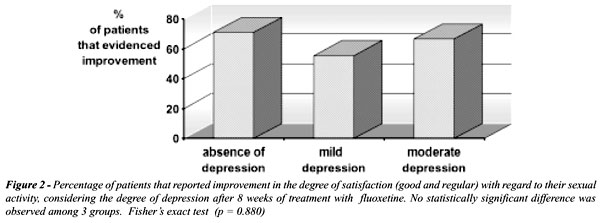
It was observed that the improvement occurred
independently from the initial anxiety level (Figure-1) and depression
(Figure-2).
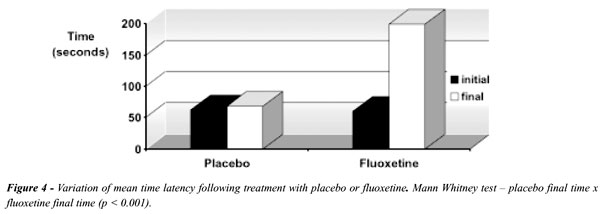
The results of latency time are shown in
table 5. Patients using fluoxetin achieved mean final latency time of
199.3 seconds, while patients using placebo achieved 68.1 seconds. The
comparison between theses times reveled a statistically significant difference
(p < 0.001).
The side effects observed, with fluoxetin
and placebo use, are demonstrated in Table-6. There was a statistically
significant difference, with higher incidence in the fluoxetin group,
of drowsiness (p = 0.002) and headache (p = 0.03).
DISCUSSION
Serotonine
(5-hydroxytryptamine, or 5-HT) is an amine formed from tryptophan, an
essential aminoacid. It acts as a neurotransmitter, almost exclusively
in the mesencephalon, pons and bulb. Its action in the central nervous
system involves the regulation of the cerebral blood flow and sleep, tolerance
to persistent stress, behavioral and impulsiveness inhibition. Its liberation
is stimulated by aversive events, leading to the regulation of defensive
behavior and/or anxiety. Besides, it is the neurotransmitter of the pain
inhibitor descendent ducts to the spinal cord (14).
The way serotonin interferes in ejaculation
is still not well-known. Svensson & Hanson (15) demonstrated that
this amine causes, experimentally in rats, ejaculation inhibition through
central and spinal ducts.
Ejaculation is a phenomenon periferically
mediated by alpha-1 noradrenergic stimulation, probably with colinergic
influence. The selective serotonin re-uptake inhibitors do not have sympathicolitic
effects not even over the parasympathetic. Therefore, the effects of these
drugs in delaying ejaculation must occur in the central nervous system
(16,17).
Adler-Graschinsky et al. (18) believe that
serotonin has an inhibitory role over the noradrenergic mechanism of the
orgasm, by inhibiting the presynaptic neuron, which facilitates the simpathetic
neurotransmission, that is, it inhibits the sympathetic nervous system,
delaying ejaculation.
Ertekin et al. (19) concluded that there
are evidences that the premature ejaculators are unable to maintain the
regional depression of the adrenergic activity during erection. Thus,
the lack of serotonin would impede the regional depression of the adrenergic
activity, allowing the ejaculation. The replacement of serotonin obtained
with the fluoxetin use would revert this situation.
This would justify the results obtained
in the present study, where the level of satisfaction with sexual intercourse
with the use of fluoxetin hydrochloride was significantly different from
the use of placebo (Figure-3).
When we evaluate the latency time, this
fact is even more evident. A statistically significant difference between
the results obtained by patients using fluoxetin and placebo was observed
(Figure-4).
Like Metz et al. (20), we believe that “the
pharmacological agents can offer hope to some men particularly those who
have a physiologic predisposition to PE”.
CONCLUSIONS
Fluoxetin hydrochloride is effective in the treatment of primary PE, increasing ejaculatory latency time with minor and temporary side effects. The improvement occurs independently from patients anxiety level or depression and independently from an improvement in those aspects.
____________________________
FARMASA laboratory has provided
the fluoxetin and the placebo used in this study
REFERENCES
- Spector IP, Carey MP: Incidence and prevalence of the sexual dysfunctions: a critical review of the empirical literature. Arch Sex Behav, 19: 389-408, 1990.
- Waldinger MD, Hengeveld MW, Zwinderman AH: Ejaculation-retarding properties of paroxetine in patients with primary premature ejaculation: a double-blind, randomized, dose-response study. Br J Urol, 78: 592-595, 1997.
- Strassberg DS, Mahoney JM, Schaugaard M, Halev E: The role of anxiety in premature ejaculation: A psychophysiological model. Arch Sex Behav, 19: 251-259, 1990.
- Althof SE, Levine SB, Corty EW: A double-blind crossover trial of clomipramine for rapid ejaculation in 15 couples. J Clin Psychiatry, 56: 402-407, 1995.
- Schover LR, Friedman JM, Weiler SJ, Heiman JR, Lopiccolo J: Multiaxial problem-oriented system for sexual dysfunction. Arch Gen Psychiat, 39: 614-619, 1982.
- Cooper A, Cernovsky ZZ, Colussi K: Some clinical and psychometric characteristics of primary and secondary premature ejaculators. J Sex Marital Ther, 19: 276-288, 1993.
- Costa M: Ejaculação precoce: os minutos que valem ouro. Urol Contemp, 3: 81-86, 1997.
- Kaplan HS: A Nova Terapia do Sexo. Rio de Janeiro, Nova Fronteira, p. 75, 1974.
- Masters WH, Johnson VE: A Incompetência Sexual. Rio de Janeiro, Civilização Brasileira, pp. 93-95, 1979.
- McMahon CG: Treatment of premature ejaculation with sertraline hydrochlorider: a single-blind placebo controlled crossover study. J Urol, 159: 1935-1938, 1998.
- Schapiro B: Premature ejaculation: a review of 1130 cases. J Urol, 50: 374-379, 1943.
- Bennett D: Letter to editor on use of MAOIs for premature ejaculation. Lancet, 2: 1309, 1961.
- Haensel SM, Klem TM, Hop WC, Slob AK: Fluoxetine and premature ejaculation: a double-blind, crossover, placebo controlled study. J Clin Psychopharmacol, 18: 72-77, 1998.
- Graeff FG, Brandão ML: Neurobiologia das Doenças Mentais. São Paulo, Lemos Editorial e Gráfica Ltda, pp. 45-46, 1993.
- Svensson L, Hanson S: Spinal monoadrenergic modulation of masculine copulatory behaviour in the rat. Brain Research, 302: 302-315, 1984.
- Segraves RT: Effects of psychotropic drugs on human erection and ejaculation. Arch Gen Psychiat, 46: 275-284, 1989.
- Waldinger MD, Berendsen HHG, Blok BFM, Olivier B, Holstege G: Premature ejaculation and serotonergic antidepressant-induced delayed ejaculation: the involvement of serotonergic system. Behav Brain Res, 92: 111-118, 1998.
- Adler-Graschinsky E, Butta NV, Elgoyhen AB: Serotonin uptake inhibitors and the prejunctional effects of serotonin on peripheral sympathetic nerves. Life Sci, 39: 61-68, 1986.
- Ertekin C, Çolakaglu Z, Altay B: Hand and genital sympathetic skin potentials in flaccid and erectile penile states in normal potent men and patients with premature ejaculation. J Urol, 153: 76-79, 1995.
- Metz ME, Pryor JL, Nesvacil LJ, Abuzzahab F, Kosnar J: Premature ejaculation: a psychophysiological review. J Sex Marital Ther, 23: 3-23, 1997.
_______________________
Received: October 11, 2001
Accepted after revision: March 1, 2002
_______________________
Correspondence address:
Dr. José Pedro Trevisan Novaretti
Rua Carlos Botelho, 520
Marília, SP,17516-190, Brazil
Fax: + + (55) (14) 422-3600
E-mail: novaretti@terra.com.br