CLINICAL
AND URODYNAMIC EVALUATION IN WOMEN WITH STRESS URINARY INCONTINENCE TREATED
BY PERIURETHRAL COLLAGEN INJECTION
(
Download pdf )
S.B. MARTINS, E. OLIVEIRA, R.A. CASTRO, M.G. SARTORI, E.C. BARACAT, G.R. LIMA, M.J. GIRAO
Department of Gynecology, Federal University of Sao Paulo, UNIFESP, Sao Paulo, SP, Brazil
ABSTRACT
Objective:
To evaluate the success of treatment with periurethral collagen injections
in patients suffering from stress urinary incontinence (SUI) with bladder
neck hypermobility and intrinsic sphincter deficiency.
Materials and Methods: Forty women suffering
from (SUI) were selected and divided into GI (consisting of 13 women with
SUI and bladder neck hypermobility) and GII (consisting of 27 women with
SUI and intrinsic sphincter deficiency). Periurethral collagen was injected
followed by a subjective evaluation (the need for urinary protectors)
and an objective evaluation through urodynamic study before and after
the treatment.
Results: It was noticed that after 9 months
there was a decrease in the need of urinary protectors in the two groups.
It was observed through the urodynamic study that either cure or improvement
was achieved in 46% in GI and 40.7% in GII. There was a significant increase
in the leak pressure in GII. Moreover, there was a decrease in the volume
of urine leak in the two groups, being the results in GII statistically
significant.
Conclusions: It was concluded that the periurethral
collagen injection is useful for the treatment of the SUI. The results
in hypermobility are similar to those in intrinsic sphincter deficiency.
In fact, it is a very simple out patient’s procedure, with little
side effects.
Key
words: urinary incontinence, stress; urinary sphincter; injections;
collagen
Int Braz J Urol. 2007; 33: 695-703
INTRODUCTION
In
its latest publication, the ICS (International Continence Society) defines
the urinary incontinence as the complaint of any involuntary leakage of
urine. The stress urinary incontinence (SUI) is the complaint of involuntary
leakage on effort or exertion, or on sneezing or coughing. It is the most
common type of urinary incontinence (1).
The stress urinary incontinence affects
10% to 30% of women above 50 years of age. Patients with intrinsic sphincter
deficiency (ISD) present high grade stress urinary incontinence and have
low abdominal leak point pressures on urodynamic studies. On the other
hand, those with bladder neck hypermobility present low grade stress urinary
incontinence (2).
Periurethral injection is being used for
almost one century for the treatment of stress urinary incontinence. Several
substances have been employed, and among them Teflon, autologous fat,
silicone micro-implants, Durasphere, Zuidex and bovine collagen (2-4).
The injection aims at increasing urethral strength, avoiding thus urinary
leak.
Periurethral collagen injection (PCI) has
been used in the treatment of SUI due to intrinsic sphincter deficiency
since 1993 when it was first approved for this application by the U.S.
Food and Drug Administration (5).
It has been reported that stress urinary
incontinence associated to intrinsic sphincter deficiency can be treated
with reasonable success by means of periurethral collagen injections (6).
However, periurethral collagen injections
have also been efficacious in patients with bladder neck hypermobility.
The use of collagen in bladder neck hypermobility was evaluated in a nonrandomized
prospective study that concluded that this therapy is appropriate in those
patients who wish to avoid surgical risks and to whom surgery is ill advised
(7).
Because collagen is less invasive than surgery
(i.e., retropubic bladder neck suspension or slings), it could represent
an interesting alternative for the treatment of SUI. The side effects
of collagen injection are generally transient (e.g., urgency, frequency
syndrome, retention) (7,8).
Long-term outcomes for the most commercially
available bulking agents including collagen demonstrate a cure rate of
25% to 45% and an improvement rate of 25% to 70%. However, due to the
decreased effectiveness of collagen with time, repeating injections may
be necessary (9).
Most of the studies demonstrate that patient
selection is important in the outcomes with PCI. The ideal patient should
have diminished urethral function with minimal proximal urethral hypermobility
(10).
Thus, in the world literature there is no
consensus of opinion that patients with hypermobility will not benefit
from PCI.
We evaluated women with SUI with hypermobility
and intrinsic sphincter deficiency treated with PCI through clinical criteria
(number of urinary protectors) and urodynamic parameters.
MATERIALS AND METHODS
Between
January 2004 and January 2005 40 women with stress urinary incontinence
were studied: 13 with bladder neck hipermobility (GI) and 27 with intrinsic
sphincteric deficiency (GII).
All patients underwent a meticulous baseline
evaluation, including a complete history, physical examination and urine
culture.
They also underwent a urodynamic evaluation
that confirmed the diagnosis of stress urinary incontinence in both groups.
The urodynamic evaluation was repeated four months after the PCI.
In GII, the ISD was defined as an VLPP of
less than 60 cm H2O. Bladder neck displacement greater than 10 mm measured
by transperineal ultrasound was used to define bladder neck hipermobility
in GI.
The age ranged from 36 to 81 (mean of 60.4).
Age was homogeneous between GI and GII. The groups were also homogeneous
as to the number of previous surgeries for stress urinary incontinence.
Women who presented contraindications to
collagen injections (allergic reaction) were excluded. Subjects with neurogenic
bladder, interstitial cystitis and pelvic prolapse higher than stage II
were also excluded.
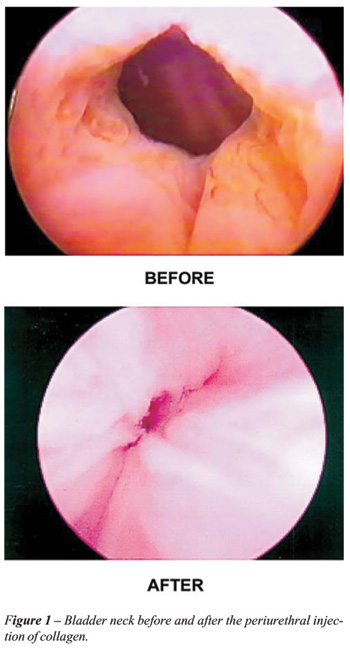
It was agreed that intraurethral collagen
submucosal injection under local anesthesia (3 to 4 mL xylocaine 1%) as
an outpatient procedure would be used for all patients. Collagen was injected
at the 3-o’clock, and 9-o’clock positions until coaptation
of the urethral mucosa was obtained (Figure-1). Sequential injections
were given 1 month apart until continence was achieved or until it was
predicted that further injections would not provide success. Follow-up
visits were conducted at 1, 3, 4, 6 and 9 months after collagen injection.
The success of the intervention was evaluated
by means subjective and objective criteria (number of urinary protectors
and urodynamic parameters respectively).
Cure was defined as the absence of urine
leak during cistometry performed four months after collagen periurethral
injections, improvement when there was urine leak with a volume 50% bigger
than those before treatment and we consider failure when the urine leak
occurred with a volume similar to that before PCI.
The study was approved by the Medical Ethics
Committee of the Federal University of Sao Paulo, Escola Paulista de Medicina.
All patients gave informed consent to participate in the study.
Statistical analysis was performed with
the software Analyze-it® for Microsoft® Excel. Statistical significance
of differences among the number of urinary protectors, Valsalva leak point
pressure, maximum urethral closure pressure and volume of urine leak before
and after PCI were assessed using non-parametric tests (Kruskal-Wallis
or Mann-Whitney tests, as appropriate). The occurrence of the cure, improvement
or failure was assessed using chi-square test. P < 0.05 was considered
statistically significant.
RESULTS
The
need to use urinary protectors before treatment in GI was smaller than
GII. However, after the treatment it was similar in the two groups (Figure-2).
It was noticed that after 9 months there
was a significant decrease in the need to use urinary protectors in the
two groups. (Figure-3).
It was observed through the urodynamic study
that either cure or improvement was achieved in 46% in GI and 40.7% in
GII (p > 0.05) (Table-1).
There was an increase in the leak pressure
in both groups, but it was significant only in GII (Graphic-2). We also
compared the maximum urethral closure pressure (MUCP) in both groups before
and after the treatment with periurethral collagen injections and we could
not find significant differences (Figure-4).
Besides, there was a decrease in the volume
of leakage of urine during urodynamic evaluation in the two groups, being
the results in group II statistically significant (Figure-5).
In our series additional injections were
given in seven cases of GI and fifteen of GII (p > 0.05). As for the
volume of injection, there were no differences between GI and GII.
As far as side effects are concerned, there
was no case of urinary retention. There was a case of urinary infection
in GI and another in GII, both were successfully treated.
COMMENTS
Collagen
is a popular, safe and effective periurethral bulking agent for the treatment
of stress urinary incontinence primarily due to intrinsic sphincter deficiency.
The procedure may be done under local anesthesia,
the period of convalescence is short, and complications are minimal (11).
The reported success rate of collagen injection
varies considerably according to patient selection and follow-up duration
and also according to the investigator definition of cure, improvement
and failure.
There has been a previous collagen outcome
assessed by direct patient questioning on symptom severity and pad requirements
(12,13). The outcome reported cure in 23% to 74% of cases, improvement
in 20% to 52% and failure in 6% to 33%.
Our results are similar from those concerning
the cure and improvement rates in the world literature. However, we believe
that most cases reported as cured in previous studies would be reclassified
as improved by our strict criteria. Moreover, cure should imply the reestablishment
of normal voiding patterns but in most studies cure denotes that the patient
no longer had stress urinary incontinence. Thus, in most cases our new
onset urge incontinence, urinary urgency or difficult voiding may have
been present.
As opposed to these favorable long-term
results, collagen injection is not considered to be a durable procedure
and most patients need additional treatment sessions to achieve and maintain
improvement or cure. In our series in seven cases additional injections
were given in GI and fifteen in GII (p > 0.05). In addition, there
have not been differences of injection volume between the two groups.
Our study observed a graduated increase
of the need of urinary protectors through consecutive months after PCI
(Graphic-1). This can be an evidence of the low durability of this procedure.
We also observed urodynamic parameters that
have denoted that PCI can be useful in SUI with intrinsic sphincter deficiency.
In this group there was a significant increase of the VLPP (Graphic-2).
This finding was also reported by other authors (14,15). Overall the literature
is inconclusive on the association of improved incontinence grade and
increased leak point pressure after treatment as well as the predictive
nature of baseline leak point pressure (7).
Among some of the issues addressed in this
paper there are the value of collagen injections in patients with hypermobility
and ISD. Regarding hypermobility, ISD became the sole indication for the
use of collagen in patients with stress urinary incontinence as a result
of the US multicentric trial (16). Since then a number of reports have
demonstrated the use of collagen in patients with hypermobility. Herschorn
& Radomski (17) found no difference in outcomes with stress urinary
incontinence with hipermobility and ISD. The series of Moore et al. (18)
included patients with both types of SUI.
In the editorial by McGuire & Appell
(6), the results at more than 1 year in women with ISD were statistically
similar to those in women with hypermobility, although Appell (19) subsequently
reported that the all patients with hypermobility required bladder neck
surgery with 2 years.
In our study, we found similar decrease
in the need to use urinary protectors in both groups. Moreover, cystometric
evaluation allowed us to infer that outcome results for hypermobility
or ISD are similar.
Therefore, in the light of these several
recent studies, including our own, we concur that urethral hypermobility
is not a contraindication to injection therapy.
CONCLUSIONS
In our series either cure or improvement was achieved in 46% of the patients in GI and 40.7% in GII. Therefore, periurethral collagen injection may provide a minimally invasive means to treat both types of stress urinary incontinence. We concur that bladder neck hypermobility is not a contraindication to injection therapy.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, et al.: The standardisation of terminology in lower urinary tract function: report from the standardisation sub-committee of the International Continence Society. Urology. 2003; 61: 37-49.
- Appell RA: Valsalva leak point pressure (LPP) vs. urethral closing pressure profile (UPP) in the evaluation of intrinsic sphincter deficiency (ISD). Presented at annual meeting of American Urogynecology Society, Toronto, Ontario, Canada, September. 1994; pp 21-4.
- Lightner D, Calvosa C, Andersen R, Klimberg I, Brito CG, Snyder J, et al.: A new injectable bulking agent for treatment of stress urinary incontinence: results of a multicenter, randomized, controlled, double-blind study of Durasphere. Urology. 2001; 58: 12-5.
- Chapple CR, Haab F, Cervigni M, Dannecker C, Fianu-Jonasson A, Sultan AH: An open, multicentre study of NASHA/Dx Gel (Zuidex) for the treatment of stress urinary incontinence. Eur Urol. 2005; 48: 488-94.
- Kershen RT, Dmochowski RR, Appell RA: Beyond collagen: injectable therapies for the treatment of female stress urinary incontinence in the new millennium. Urol Clin North Am. 2002; 29: 559-74.
- McGuire EJ, Appell RA: Transurethral collagen injection for urinary incontinence. Urology. 1994; 43: 413-5.
- Bent AE, Foote J, Siegel S, Faerber G, Chao R, Gormley EA: Collagen implant for treating stress urinary incontinence in women with urethral hypermobility. J Urol. 2001; 166: 1354-7.
- Corcos J, Collet JP, Shapiro S, Herschorn S, Radomski SB, Schick E, et al.: Multicenter randomized clinical trial comparing surgery and collagen injections for treatment of female stress urinary incontinence. Urology. 2005; 65: 898-904.
- Shortliffe LM, Freiha FS, Kessler R, Stamey TA, Constantinou CE: Treatment of urinary incontinence by the periurethral implantation of glutaraldehyde cross-linked collagen. J Urol. 1989; 141: 538-41.
- Dmochowski RR, Appell RA: Injectable agents in the treatment of stress urinary incontinence in women: where are we now? Urology. 2000; 56: 32-40.
- Appell RA: Collagen injection therapy for urinary incontinence. Urol Clin North Am. 1994; 21: 177-82.
- Winters JC, Chiverton A, Scarpero HM, Prats LJ Jr: Collagen injection therapy in elderly women: long-term results and patient satisfaction. Urology. 2000; 55: 856-61.
- Cross CA, English SF, Cespedes RD, McGuire EJ: A followup on transurethral collagen injection therapy for urinary incontinence. J Urol. 1998; 159: 106-8.
- Smith DN, Appell RA, Winters JC, Rackley RR: Collagen injection therapy for female intrinsic sphincteric deficiency. J Urol. 1997; 157: 1275-8.
- Herschorn S, Radomski SB, Steele DJ: Early experience with intraurethral collagen injections for urinary incontinence. J Urol. 1992; 148: 1797-800.
- Elsergany R, Elgamasy AN, Ghoniem GM: Transurethral collagen injection for female stress incontinence. Int Urogynecol J Pelvic Floor Dysfunct. 1998; 9: 13-8.
- Herschorn S, Radomski SB: Collagen injections for genuine stress urinary incontinence: patient selection and durability. Int Urogynecol J Pelvic Floor Dysfunct. 1997; 8: 18-24.
- Moore KN, Chetner MP, Metcalfe JB, Griffiths DJ: Periurethral implantation of glutaraldehyde cross-linked collagen (Contigen) in women with type I or III stress incontinence: quantitative outcome measures. Br J Urol. 1995; 75: 359-63.
- Appell RA: Periurethral injection therapy. In: Walsh PC, Retik AB, Vaughan ED, et al.: (ed.), Campbell’s Urology, 7th ed. Philadelphia, WB Saunders. 1998, pp. 1109-20.
____________________
Accepted after revision:
April 25, 2007
_______________________
Correspondence address:
Dr. Sérgio Brasileiro Martins
Rua Hélio Pelegrino, 250 Ap. 112
São Paulo, SP, 04513-100, Brazil
E-mail: emerson_oliveira@terra.com.br
EDITORIAL COMMENT
The
authors present their results of periurethral collagen injections in 27
women with stress urinary incontinence.
Most
studies to date have some urodynamic outcomes included. Most are also
of longer duration. It is not clear from the introduction just what question
the authors want to address.
It
is also not mentioned whether patients were given additional injections.
It is well known that injectables, especially collagen, may require a
few initial sessions for success. If this was not done, it may have compromised
the continence outcome.
Regarding
the treatment outcomes, the demonstrated leak on cystometry is understood,
but there are many patients who do not leak with catheters in place. Do
they possibly mean a cough-stress test as an outcome measure? Furthermore,
what do they mean by volume of leakage? Is it volume in the bladder at
which the leakage occurred? If so, then they should provide evidence that
this test has been validated and standardized as an outcome measure.
It
appears that the results of treatment in both groups are similar, despite
the pre-treatment testing, and despite some discrepancies in urodynamic
results.
In
the Comments, the authors point to discrepancies between their results
and previously published outcomes. From the data they present, the success
rates appear relatively similar. Longer term results are mostly less favorable
than short-term results. Furthermore, there are clinical outcome measures
that are valid in SUI studies. This study has no clinical outcome measures,
e.g. validated questionnaires, against which to compare the urodynamic
results.
The
authors indicate the lack of durability as evidenced by the increasing
need for pads. They then state that collagen can be useful in SUI with
ISD. However, they actually showed that the results in patients with normal
sphincters (GII?) were the same.
Dr. Sender
Herschorn
Sunnybrook and Women’s College
Health Sciences Center
Toronto, Ontario, Canada
E-mail: s.herschorn@utoronto.ca
This looks at 40 women suffering from stress urinary incontinence over a one-year period. It is not clear on what basis patients were differentiated into the group with intrinsic sphincter deficiency and those with normal sphincters – it is a very vague area and it is difficult to separate out the groups. Clearly though it is a consecutive series followed up prospectively – the authors do not mention Zuidex, which is a new agent, which has been around for some time now, and this is an oversight in their literature survey.
Under results, it is interesting to see that there is limited cure shown urodynamically.
Dr. Christopher R. Chapple
Department of Urology
Royal Hallashire Hospital
Sheffield, United Kingdom
E-mail: c.r.chapple@shef.ac.uk